
Participants in the Spring Global Health Elective. From left: Dr. James Osorio and his daughter Sophie Osorio, Dr. Grace Shih and Dr. Melvin La
In the Cornell Anesthesiology Circle of Life, interview and the annual In Training Exam are behind us, interns are closer to being done than having started, CA1s are starting to feel comfortable in their own skin as budding anesthesiologists, CA2s are going fellowship-application-crazy, and CA3s are starting to lament only four more months of their residency training!
I am spending time looking inward as we are at the beginning of our ‘Self-Study’ year; a process the ACGME mandates all programs due every 10 years that rigorously evaluates our strengths, areas for improvement, threats, and opportunities. It is a lot of work, but an excellent opportunity to formally codify processes that we constantly doing on our own – taking stock of where our residency program is, and ensuring it remains one of the top programs in the country.
A couple of near 70 degree days this past week have me looking forward to the spring. We are launching several new programs including class-wide weekend retreats away, programmatic community service opportunities, and bring your family to work day in our SAIL simulation center where significant others, children, family, and friends can learn what it is that anesthesiology residents spend all of that time in the hospitals doing. Our Global Health Division is busy working on our second international elective in Rwanda (September 2018) which brings the total number of CA3 elective participants to five annually!
Our spring elective in India is currently underway, and here is a snippet from their travel journal with accompanying pictures:
Notes from the Spring Global Health Elective
Dr. Melvin La, Chief Resident, CA3:
“This morning, we headed out before sunrise to see the Golden Temple again. We arrived around 6:30 am and were able to see the temple brightly illuminated like a brilliant gem floating in the middle of a tranquil pool. The sun coming up also cast a beautiful shine on the gold-leafed walls of the temple. This was easily my favorite sight of the trip so far.
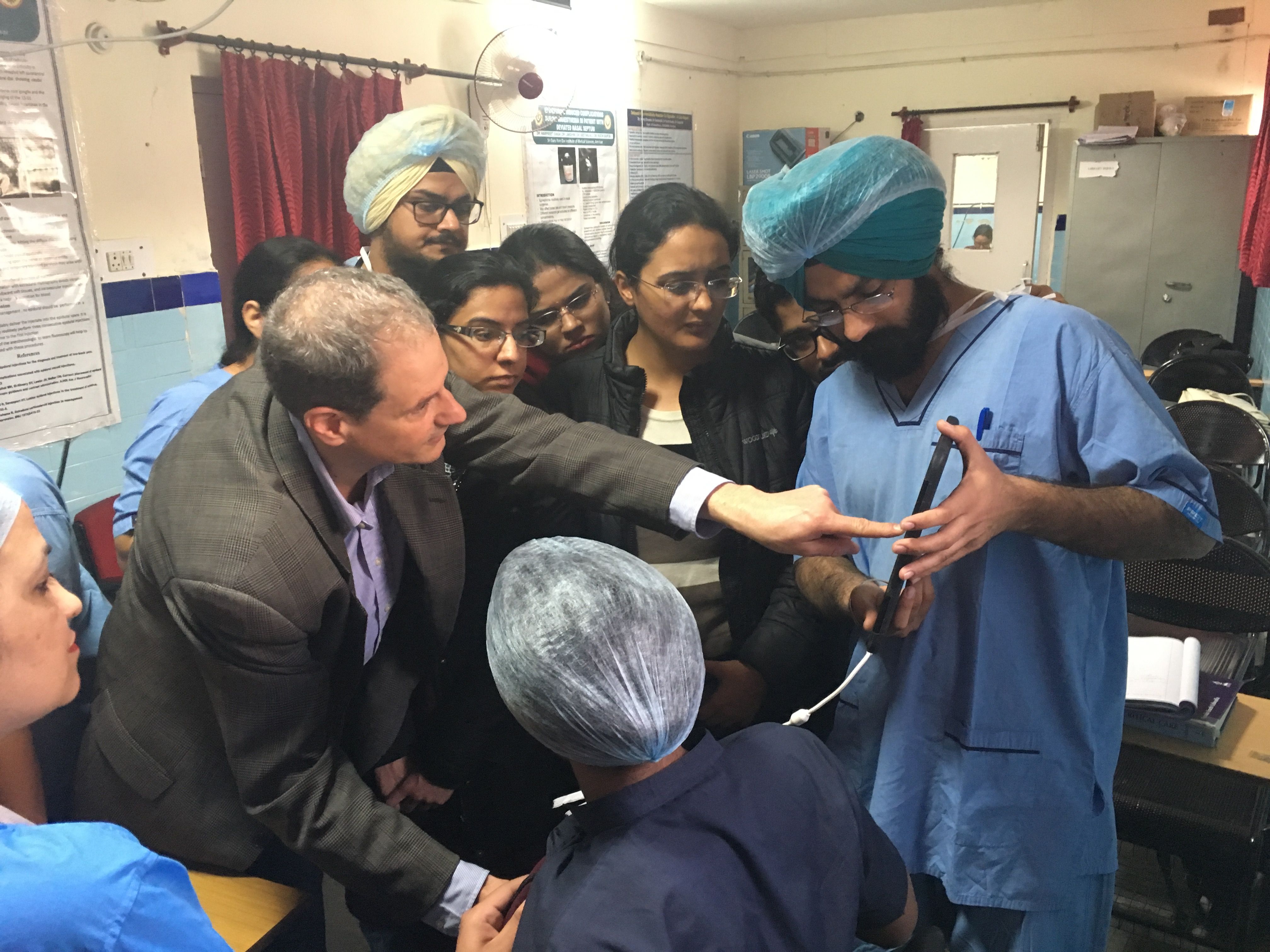
Today we returned to SGRD, where Dr. Osorio gave a talk on POC ultrasound, including the use of ultrasound for FAST, FATE, and RUSH exams. At the end of the talk, we showed the residents how to perform a basic TTE exam using a portable Phillips ultrasound probe that Dr. Osorio brought with him on the trip. The probe itself is handheld, fits in your pocket and connects to an iPad with the enabled software. We recruited a volunteer from among the OT staff who became our model and the residents took turns using the ultrasound to look for the basic echocardiogram views. The residents were clearly excited and very interested, and it was incredibly rewarding to teach them. We later went into the OTs to observe a few cases. I got to see supraclavicular block performed using landmark technique only for a humerus fracture. The technique involved palpating for the lateral border of the SCM in the supraclavicular fossa and inserting the needle pointing towards the ipsilateral nipple, feeling for two fascial “pops”. There was a little difficulty in the placement and they ended up using nearly 40cc of local but the block worked perfectly fine. I also watched a spinal anesthetic with bilateral obturator nerve blocks performed for a TURB. The obturator nerve blocks were performed using nerve stimulator technique. They used the femoral pulse and pubic tubercle as their landmarks, going halfway between them and 2cm inferior. The needle is advanced until leg adduction is elicited. Again, the patient received minimal sedation for the case, other than some midazolam and butorphanol given at the start.
Later, we visited the Wagha border ceremony. It was a decent drive from the city, about 50 minutes. I was surprised to see that the border ceremony was an incredible display of Indian nationalism and pride, akin to a July 4th celebration back home. Large crowds were gathered to watch the Indian troops march ceremoniously back and forth the border gate, exchange brisk handshakes with the Pakistani troops, and eventually lower the flag at the border gate. There was dancing, loud music, and cheers from the crowd, almost like they were watching a sporting event.”

Dr. Grace Shih, CA3, Senior Residency Support Council Member:
“Back to SGRD today. We started the day with being ushered to the academic corner of the OR, an unsubtle way of having us give a presentation--thankfully Dr. Ruchi had asked Dr. Osorio to talk about mechanical ventilation to reinforce the concept since the residents recently covered that topic over the weekend. Towards the end of that lecture, Dr. Ruchi told me about a peds case starting in OT4 so I left for that. The case was a 15-year-old boy getting a colostomy closure, so it was more a GA case of a small adult than peds, but still worth being in. I saw the “O2 pressure supply low” alarm go off for the first time. No one seemed concerned except for me--the resident said that someone was probably changing the main hospital supply O2 tank, and shortly thereafter the alarm went off on its own--it happens enough so they’ve become accustomed. I find it interesting that they often use succinylcholine as the paralytic of choice for intubation, and afterward will maintain paralysis with vecuronium or atracurium. They don’t have train of four monitoring, so per the resident, they reverse based on clinical symptoms; they are hand ventilating the entire time (Dr. Ruchi’s order for the residents, so that they have practice for the future when they have ventilators that don’t function) so they can start sensing when the patient is starting to breathe, though I did notice that they tend to hyperventilate while handbagging. Similar to when we do peds cases, the drugs are weight-based and the resident often has written out a list of the meds and their doses and expected the amount to give based on a patient’s weight. Some things are the same no matter where you are.
I stayed only for the start of the case and then went to catch up with the rest of the group who had gone down to the ICU. The ICU at SGRD is an open system ICU, where beds are only separated by a curtain. Before entering the ICU, we all put on green gowns, caps, and masks (mostly as PPE)--also which I remember doing when I was doing my medical school rotation in China. The walk through the ICU was pretty interesting; the ICU consultant and residents were quite interested in Dr. James’s input as they walked around the ICU. The patients there were definitely sick, and the staffing similar.
After that tour, we sat in Dr. Ruchi’s office for chai and to chat with her more about her residency program, education, and whatnot. Dr. Ruchi is a fantastic attending--she really cares about her residents, and takes special care of her “turtles” (the residents that look extra lost, but ones that she knows will work harder than the rest because they feel like they are behind, and eventually turn out to be the better clinicians). I can see that she thinks a lot about resident education, and how to constantly make the experience more worthwhile for them."
E.B